

Not a heart attack!
Heart attack and cardiac arrest: two very different beasts that require different courses of treatment.

For the thousandth time, I did not have a heart attack.
I am addressing this in an early post because most of us don’t know the difference. I sure didn’t, until I survived one and not the other. Now, when I tell someone what happened, they usually refer to my medical event as a heart attack—often, in the very next sentence after I tell them it was a cardiac arrest.

Sudden cardiac arrest is not another term for heart attack. Cardiac arrest is not a type of heart attack. Many cardiac arrests have nothing to do with heart attacks. The risk profiles for both are quite different. Cardiac arrest and heart attack do both involve the heart—and that’s all they necessarily have in common.
Importantly, these two distinct medical events require drastically different responses from bystanders. Around 80% of cardiac arrests occur outside a hospital. Victims die within a few minutes unless someone nearby takes action. Knowing the difference between a heart attack and cardiac arrest could help you save a loved one’s life.
Here’s an essential breakdown:
Heart Attack:
The victim is awake! Their heart is beating. They may complain about a range of symptoms (such as chest or jaw pain and shortness of breath) that come and go over minutes, hours, or even days. Call 911 or get the person to the hospital. You want to get this checked out, especially if the victim is in a high risk category (e.g. they smoke, have high blood pressure, have diabetes, aren’t very physically active, or have a family history of heart disease).
Cardiac Arrest:
The victim is unconscious and their heart is not beating. Their organs are shutting down due to lack of oxygen. The brain will be the first to go. You may see some convulsions as the brain stops receiving blood from the heart. You’re in a race against brain death, and seconds matter.
Note: A cardiac arrest victim is clinically dead. “Your actions can only help.” So call 911 and start CPR. If there are multiple people present, one should start CPR while another calls 911.
I am cognitively intact because my husband heard me having a seizure and came to my aid. Then, he saw my lips turn blue. He called 911 and started CPR. He was not certified—he just worked hard until EMTs arrived.
Fast forward to my first cardiology follow-up one week after ICU discharge. I hobbled into the clinic and there it was, emblazoned above the check-in desk:
“HEART FAILURE”
I’d just survived cardiac arrest. My heart had required four hits with the paddles to get going again. Over a couple weeks, my ejection fraction rebounded from 15% to near 40%. My heart may have failed temporarily, but then it started winning! Now I had a personal shock box (subcutaneous defibrillator or S-ICD) implanted in my chest. I felt invincible. “Heart failure” was a downer of a diagnosis to be awarded after going through so much and coming out on top.
I asked my cardiologist, a heart failure specialist, whether I was being branded with a new chronic condition on top of my existing epilepsy. I didn’t receive a straight answer. It’s early days, I reassured myself mentally. The doctors need more data. And I need to get stable.
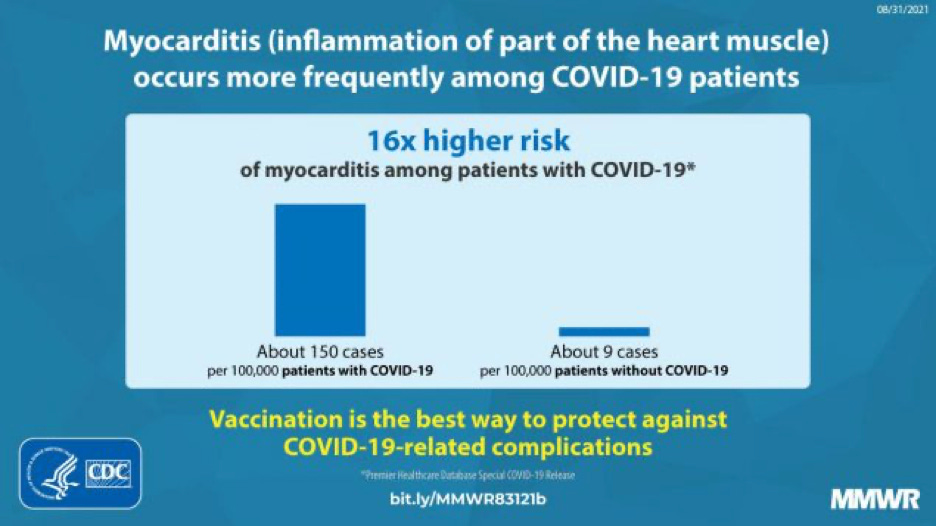
The one thing we did know was that my cardiac arrest was most likely attributable to acute myocarditis. I had an active COVID-19 infection while in the ICU. [I created a timeline of events here. For more about the connection between COVID, myocarditis, and cardiac arrest, read this article.]
I recovered from COVID while in the ICU; then, I recovered from myocarditis. In a few months, my heart ejection fraction increased to 45-50%, or “low-normal.” So I’m no longer classified as a cardiologic “failure.” Right?
Wrong.
Heart failure is one of those things you get branded for life, like epilepsy. Too big or too bad a thing happens, and nobody will ever risk being the doctor who removes the label or takes you off the meds. Some diagnoses are sticky. The best one can hope for in heart failure is temporary remission from sudden cardiac death. I know from an echocardiogram five years ago that my ejection fraction used to be 65%, so the latest reading of 45-50% may be classified as the low side of normal, but it’s not my normal. Which explains my pathetic stamina hiking and muscle fatigue after yoga these days. Don’t get too comfortable, doctors warn. “Your heart will never go back to the way it was,” cardiologist after cardiologist informs me. “You’ll need the four pillars of heart failure therapy for life.”
Something doesn’t sit right with me about this aggressive pharmaceutical approach. Unlike someone who, say, had symptoms of congestive heart failure for a while, had many of the risk factors, and was diagnosed based on reduced ejection fraction, my heart was doing just fine until I got COVID and suffered sudden cardiac arrest. I continue to struggle to find articles about any standard treatment for heart failure diagnosed after surviving cardiac arrest. Especially cardiac arrest survivors who have epilepsy. From what I can tell, I’m prescribed the exact same drugs I would be prescribed if I had suffered…
You guessed it. A heart attack.
Now, some cardiac arrests are caused by heart attacks. And most people who go into cardiac arrest die, which makes it hard to do studies on them. The longterm survival rate for a heart attack is about 97-98%; with cardiac arrest, it’s about 50%. (Source) So, it’s a lot easier to do studies on heart failure patients who are heart attack survivors. About half of cardiac arrest survivors are severely brain damaged and presumably don’t get much of a say in their medication regimen. Cardiologists probably don’t see a lot of females in their late thirties who suffer cardiac arrest during a virus, mostly recover, and then end up cognitively intact enough to want to feel like themselves again.
My blood pressure naturally runs low. It always has. It's one of the many ways I don’t fit the typical profile of someone at high risk of a heart attack. I also weigh about 112 lbs. So putting me on four medications that lower blood pressure seems suspect. Putting me on medications that lower blood pressure when my left ventricle is having trouble pumping adequate blood (and therefore oxygen) to my brain seems mildly insane. I’m just a layperson here, but I know that my brain is my heart’s biggest customer. It eats up 15% of my heart’s outflow. Lack of oxygen to my brain likely caused the breakthrough seizures that occurred in the week leading up to my cardiac arrest. We’ll never know for sure—it’s just a leading theory. Given, you know, the acute myocarditis confirmed by heart MRI in the ICU…along with my confirmed history of epilepsy…along with the grand mal my husband saw me having right before I stopped breathing and we got to take that very expensive helicopter tour of the Shenandoah Valley.
The medication cocktail I was prescribed at ICU discharge in February caused my blood pressure to drop dangerously low the following week—70/40 low. I got lethargic and slurred my speech. My husband took me back to the ER. They detoxed me overnight from the heart drug Entresto (the most expensive of the four pillars, on our current health insurance), saying it was a common culprit for severe hypotension. The ER doctor also lowered my dosages on a beta blocker and MRA, two of the other pillars. The next day, I could speak and move my limbs again. Like magic.
I’ve since had issues with a couple of other heart meds. Jardiance, a SGLT2 inhibitor and newest of the four pillars, is a diabetes drug that was recently approved for treating heart failure. There are some impressive studies backing this FDA-approved usage in many people. Unfortunately, it messes with blood sugar. My body, which has always had normal blood sugar, was a bit confused about its experience on Jardiance. I was not dancing around like the people on the drug’s TV commercials. Since I’m not diabetic and my body consumes mostly produce and home cooked whole foods, being forced to pee out sugar all the time wasn’t helpful. I started losing weight and couldn’t stop, no matter how much I ate. That was fun at first, but Jardiance also led to an imbalance in my urinary tract and a permanent, low-level yeast infection. Gross. Luckily, all that cleared up quickly when I complained to a female cardiac nurse practitioner. She took me off Jardiance immediately. Unfortunately, the ACE inhibitor she replaced it with dropped my blood pressure into the danger zone again. So right now, I’m only able to handle two of the four pillars.
The problem, if I had to guess, is that I am an atypical heart failure patient. I did not have a heart attack. I’m not obese, I’m not diabetic, I don’t drink or smoke, I’m not male, I’m not over 60, and none of the pharmaceutical heart failure studies apply to me. All the forms I had to fill out before my first cardiac rehabilitation visit concerned cutting out processed foods (which I already avoid like the plague), quitting smoking (I’ve never smoked), minimizing drinking (I’ve been a teetotaler since starting epilepsy meds), reducing stress (we’re all working on this one), and not being sedentary (I was the sort of woman who regularly enjoyed 10-mile hikes before my cardiac arrest). The forms were 100% centered around heart-attack risk factors. When I asked how treatment differed for sudden cardiac arrest survivors and myocarditis recovery, I didn’t get any clear answers.
Another patient in my cardiac rehab class loved eating cinnamon buns for breakfast. The nurses tried to convince him to transition to biscuit sandwiches with eggs and meat for breakfast. I listened to their dialogue having just eaten my normal breakfast: homemade buckwheat and oat muesli with fresh blueberries and goat’s milk. While others in cardiac rehab struggled to lose weight and bring down their blood pressure, I became underweight for the first time in my life and started having new partial seizures.
A drug or treatment plan that increases someone’s survival odds a bit if they are in every way NOT ME might actually do damage if applied to the wrong person. As weeks turned to months, I could tell that the standard protocol was being slapped down with no understanding of my situation. Even when I raised concerns or reported new symptoms, up to and including convulsions, doctors didn’t budge.
Meanwhile, all focus remained on my heart. When I insisted we look into why I was having so many partial seizures, it took a primary care doctor I got randomly assigned to at a same-day sick appointment to order a brain MRI. My regular neurologist and cardiologist had not thought this was necessary.
It didn’t take much digging to discover that my greatest risk factor for cardiac events, apart from my long bout of COVID, is epilepsy. From the journal Heart in 2015:
“Epilepsy is associated with a 2.8-fold increase in sudden cardiac death risk, and use of antiepileptic medications is associated with a 2.6-fold increase in sudden cardiac death risk.”
One of the best things a cardiologist can do for my heart is to control my seizures on an antiepileptic med that’s relatively heart-friendly (this is tough, when so many aren’t). Why wasn’t there more interest in this approach? Why wasn’t there more collaboration between neurology and cardiology since I left the ICU? Could it be that if seizures were the root cause, cardiologists simply don’t see my concerns as resting in their department? And as long as they prescribe every viable heart drug that exists and put an S-ICD in my chest, they can document that they officially did their jobs? Meanwhile, the neurologists can point to COVID myocarditis and cardiac arrest and say: we had her stable before all that happened. It’s a heart thing.
I’m not saying any individual doctors are thinking these terribly dismissive thoughts. I quite like my current doctors. I’m pointing out that industrialized healthcare breaks down the complex system of the human body into over-analyzed segments. The knee-jerk reactions that result from 10-minute appointment times with specialists are nonsensical. I’ve learned that in our healthcare system, nobody but the patient is looking out for the whole. This is why I had to quit my paid full-time job to become the unpaid prime contractor of my own healthcare and make sure my “subs” start heading in a more productive direction.
For the thousandth time: I didn’t have a heart attack. I need a plan that addresses being a female, thirty-something, epileptic survivor of COVID myocarditis-induced cardiac arrest who now has improved ejection fraction, low blood pressure, a worsening movement disorder, and refractory partial seizures. Doctors might need to get a little creative to give me the care I need. That’s why I chose to collaborate with a research clinic like NIH’s NINDS. [Note: If you are similarly at your wits end about a health debacle, I recommend searching for available studies to join at ClinicalTrials.gov.]
Researchers may also think in terms of organs instead of people. But they have the time and interest to look into wicked, complex problems. Presumably, researchers will dig beyond the published studies and established ways of thinking because they’re interested in creating new knowledge. On a follow-up visit a few weeks ago, I was at the NIH Bethesda clinic for hours. I left with a new prescription to try, some potential theories, and a game plan.
When I had my third seizure that night, Chris and I were so relieved and hopeful about the NIH appointment that we joked about how I sometimes look like I’m trying to dance right before my convulsions start. I had just enough time to really ham it up and make my arm movements extra dramatic. “I just…I think I’ve always suppressed…my desire to dance!” I stammered as my speech started slurring. Then, nothing was up to me. That was one of the seizures where I ended up on the bathroom floor. But at least I went into it laughing.
Wow! You haven't lost your writing skills, and hopefully others will benefit from this incredibly thorough report of what you are going through. You are, indeed, an enigma to the health profession, but hopefully, with your determination to get "proper" treatment, you will continue to embrace life as you do, with Chris and Nosie by your side. Love and hugs to you.
Lauren! Many thanks for writing this. My thoughts are with you and I hope you’ll recover from all this 💕!